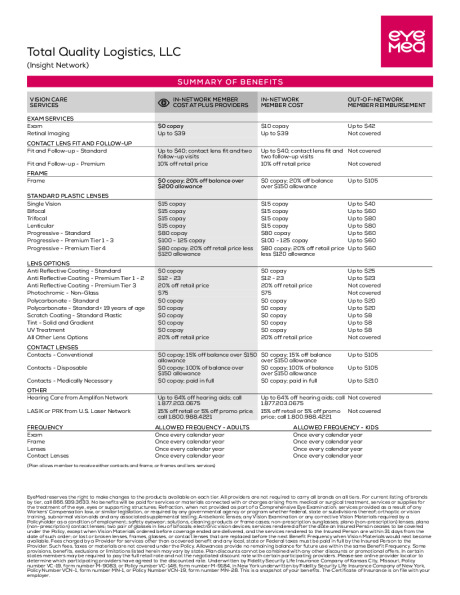
Vision Coverage Keep your vision clear with regular eye exams. Check the 2026 Benefit Summary below for in-network and out-of-network coverage. Visit our Participating Provider EYEMED online at EyeMedVisionCare.com or by calling 1-866-299-1358 Vision Plan Design & Contributions EYEMED VISION CARE Routine Exams (Annual) $10 copay, $0 for Plus Provider Lenses - Single Bifocals/TrifocalsStandard Progressive $15 Copay$80 Copay Contacts (Covered in lieu of lenses. Medically necessary contacts may be covered at a higher benefit level) $150 Allowance, 15% off balance over$150 every 12 months Frames $150 allowance (extra $50 for Plus Providers), additional 20% off balance over $150 Employee Contributions (Semi-Monthly): Vision Plan Employee $3.97 Employee & Spouse $7.12 Employee & Child(ren) $7.92 Family $11.66 EyeMed App Flyer Member Web Flyer EyeMed - 2026 Benefit Summary prevDental Telemedicinenext