
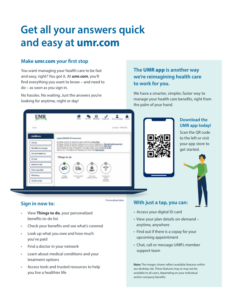
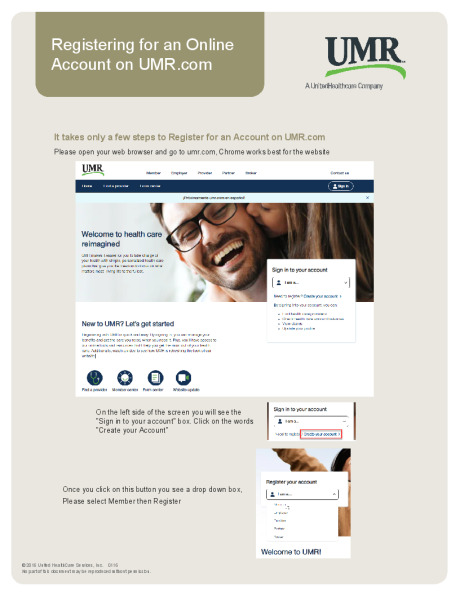
UMR Overview, Get Registered
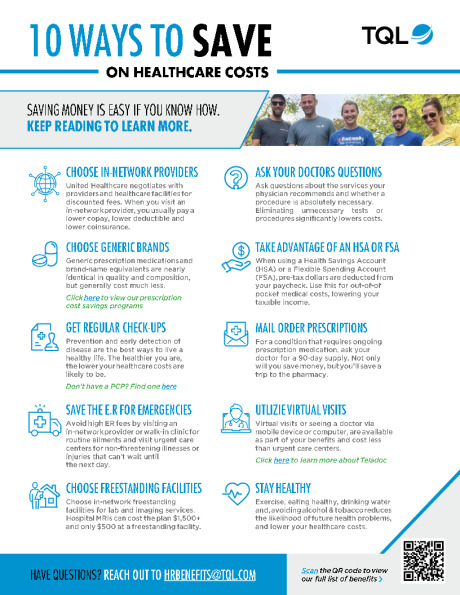
10 Tips to save on healthcare cost
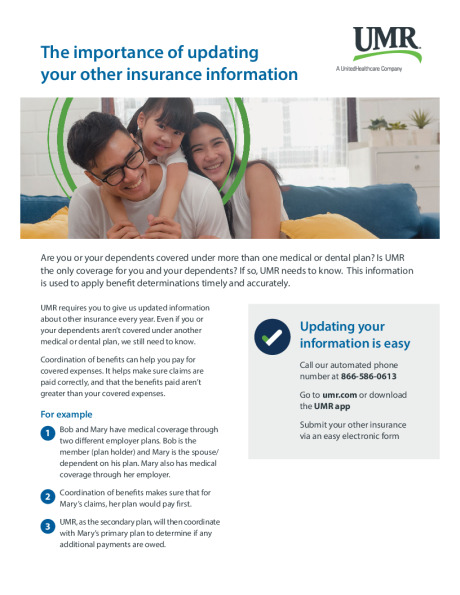
Coverage of Benefits
Call, Chat, Message
Accidents

UMR on the Go App
Securing Your Health Information
Know Where to Go
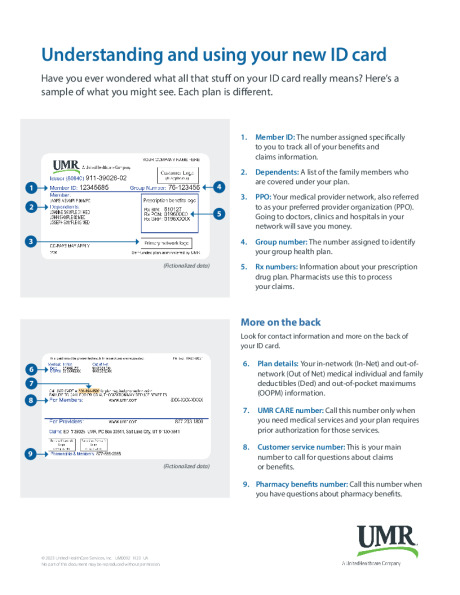
ID - Card
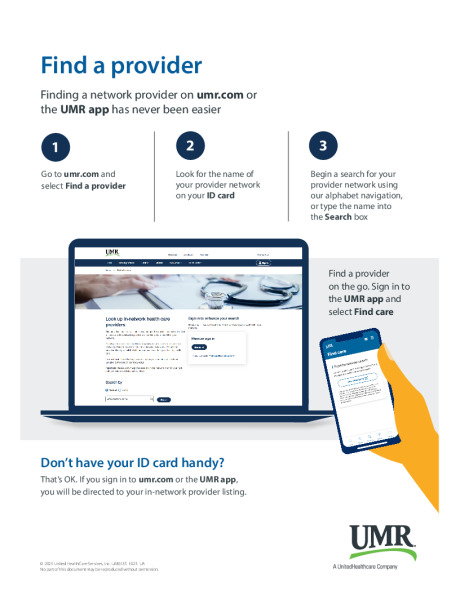
Find a Provider
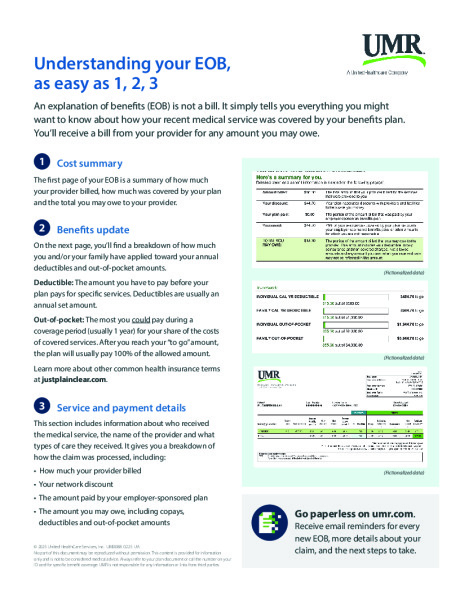
Explanation of Benefits

Learn the Language of Healthcare
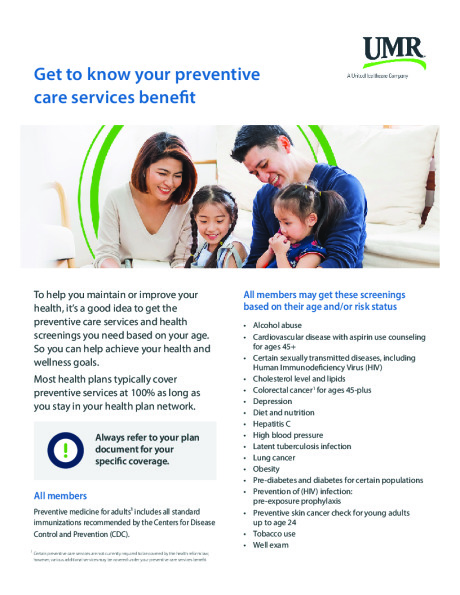
Preventative Care
CARE Support
